
Repeated number of passes, clot fragmentation, and distal embolization during mechanical thrombectomy (MT) lead to worse clinical outcomes in acute ischemic stroke. This study aimed to assess the recanalization and embolic outcomes of different stent-retrievers (SRs): open-tip SR (Solitaire X 6 × 40 mm), closed-tip SR (Embotrap II 5 ×3 3 mm), and filter-tip SR (NeVa NET 5.5 × 37 mm).
Stiff-friable clot analogy were used to create middle cerebral artery (M1-MCA) occlusions in a benchtop model. After occlusion, experiments were randomized into one of the three treatment arms. The thrombectomy technique consisted of retrieving the SR into a balloon guide catheter under proximal flow arrest and continuous aspiration. A total of 150 single-attempt cases were performed (50 cases/treatment arm). Distal emboli (>100 μm) were collected and analyzed after each experiment.
Filter-tip SR achieved a non-significantly higher first-pass recanalization rate than open-tip SR and closed-tip SR. (66% vs 48% vs 44%; P=0.064)
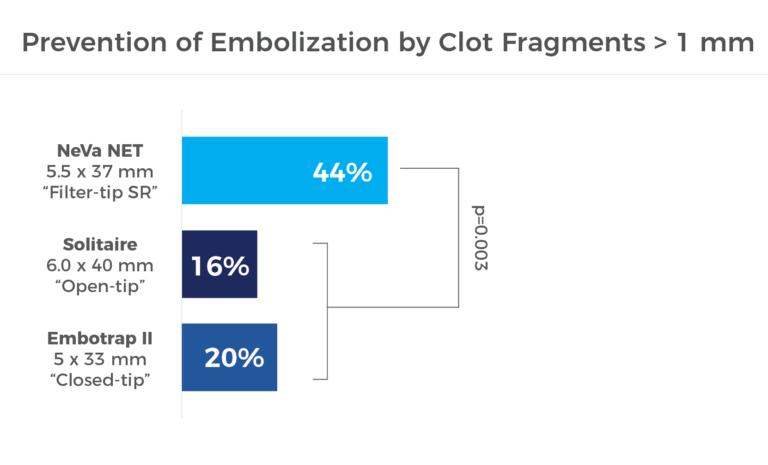
Filter-tip SR was significantly better at preventing clot fragments >1mm from embolizing distal territories. (44% vs 16% vs 20%; P=0.003)
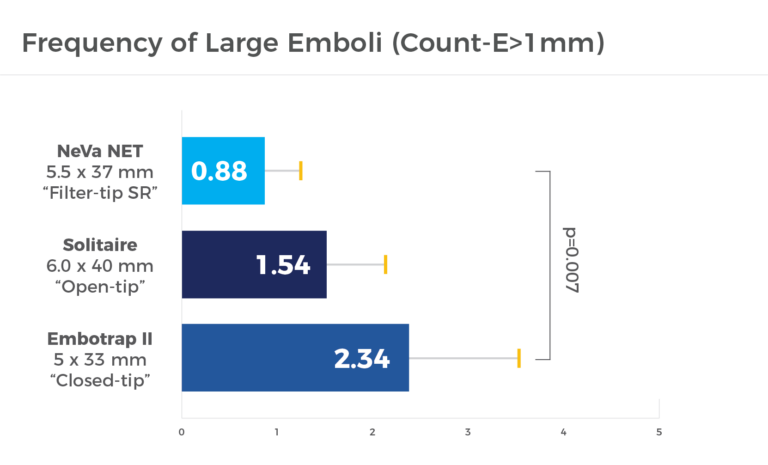
The frequency of large emboli was significantly lower in the filter-tip arm than in the closed-tip arm (count-E >1 mm=0.88±1.2 vs 2.34±3.38; P=0.007)
No significant differences were found in pairwise comparisons between open (count- E>1 mm=1.54±2.07) versus closed-tip or filter-tip SRs.
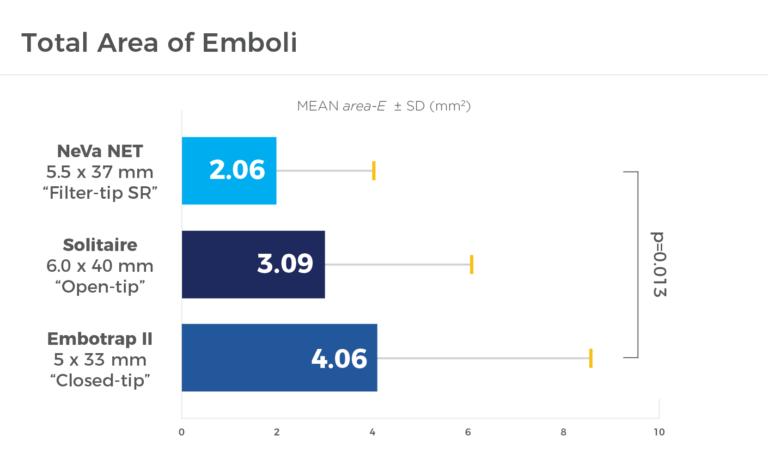
Total area of emboli was significantly smaller in the filter-tip arm than in the closed-tip arm (E=2.06±1.85 mm2 vs 4.06±4.80 mm2; P=0.013).
No significant differences were found in pairwise comparisons between open (area-E=3.09±3.12 mm2) versus closed-tip or filter-tip SRs.
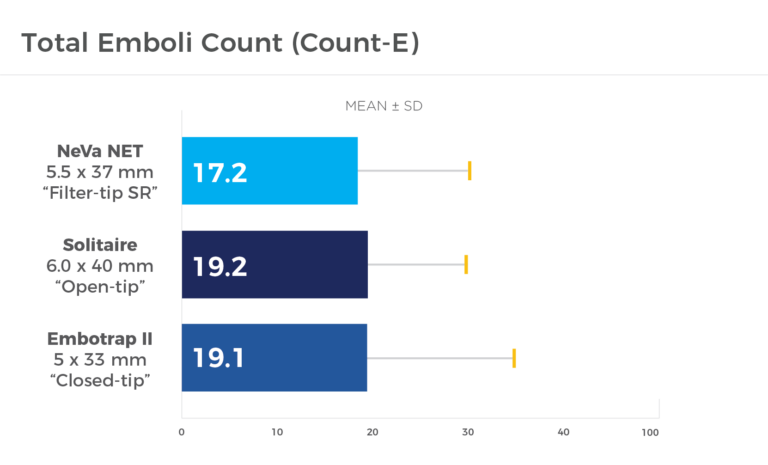
In total emboli count, the differences were not significant between treatment arms in terms of total emboli count (open-tip= 19.2±13.1, closed-tip= 19.1±10.7, filter-tip= 17.2±13.0; P=0.660).
When facing fragment-prone clots, the filter-tip SR significantly reduces the number of large clots (>1 mm) that embolize distally during an MT procedure, which in turn may increase the chances of first-pass complete recanalization.
| Cookie | Duration | Description |
|---|---|---|
| cookielawinfo-checkbox-analytics | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics". |
| cookielawinfo-checkbox-functional | 11 months | The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional". |
| cookielawinfo-checkbox-necessary | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary". |
| cookielawinfo-checkbox-others | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other. |
| cookielawinfo-checkbox-performance | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance". |
| viewed_cookie_policy | 11 months | The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data. |
by removing vascular occlusions and restoring blood flow
Please select your region to enter our world of innovation:
"*" indicates required fields